Pathophysiology
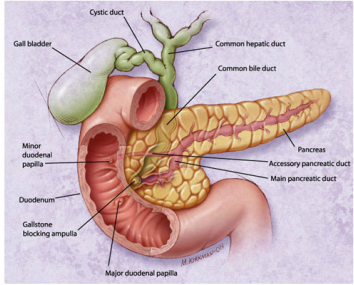
There are no ideal or consensual theories on the pathogenesis of acute pancreatitis currently available, only best guesses based on symptoms and etiology. The most common pathogenic mechanism is believed to be auto-digestion of the pancreas (Lewis et al., 2014, 1191). Auto-digestion occurs through bile-pancreatic duct obstruction, which increases pancreatic duct pressure, bile reflux, and activation of pancreatic enzymes, which are normally activated in the small intestine (Wang, Gao, Wei, Wang, & Ding, 2009, 1428). It is not clear how the activation of pancreatic enzymes occurs; one possible cause is believed to be the reflux of bile acids into the pancreatic ducts through an open or distended sphincter of Oddi (Lewis et al., 2014, 1191). The reflux may occur from gallstones blocking the ampulla or an obstruction of the pancreatic ducts themselves.
There are no ideal or consensual theories on the pathogenesis of acute pancreatitis currently available, only best guesses based on symptoms and etiology. The most common pathogenic mechanism is believed to be auto-digestion of the pancreas (Lewis et al., 2014, 1191). Auto-digestion occurs through bile-pancreatic duct obstruction, which increases pancreatic duct pressure, bile reflux, and activation of pancreatic enzymes, which are normally activated in the small intestine (Wang, Gao, Wei, Wang, & Ding, 2009, 1428). It is not clear how the activation of pancreatic enzymes occurs; one possible cause is believed to be the reflux of bile acids into the pancreatic ducts through an open or distended sphincter of Oddi (Lewis et al., 2014, 1191). The reflux may occur from gallstones blocking the ampulla or an obstruction of the pancreatic ducts themselves.
Another common cause of acute pancreatitis is excessive alcohol consumption, although it is also not entirely clear what role alcohol plays in its development. One theory is that it stimulates secretion and excess production of hydrochloric acid, which decreases the gastric pH and causes internal mucosa to release the hormone secretin. Secretin stimulates production of pancreatic secretions, resulting in auto-digestion of the gland and inflammation of neighbouring tissue (Wang et al., 2009, 1429).
The severity of acute pancreatitis ranges from edematous pancreatitis (mild and self-limiting) to necrotizing pancreatitis (the degree of necrosis correlates with the severity of manifestations) (Lewis et al., 2014, 1191).
The severity of acute pancreatitis ranges from edematous pancreatitis (mild and self-limiting) to necrotizing pancreatitis (the degree of necrosis correlates with the severity of manifestations) (Lewis et al., 2014, 1191).

Source: Medical-Surgical Nursing in Canada (2nd Ed.) 2014
Etiology
Due to its location and interaction with other organs in the epigastric region of the body, many factors can contribute to and/or cause acute pancreatitis. In Canada, the most common cause of acute pancreatitis is chronic alcohol abuse, with the second most common cause being gallbladder disease (obstruction) (Lewis et al., 2014, 1191). Less common causes include trauma, post-surgical procedures, viral infections, and metabolic disorders, or pancreatitis can also be idiopathic (unknown cause) in nature.
Incidence, Prevalence, and Developmental Concerns
Pancreatitis affects 1 million Canadians, with 600,000 Canadians currently living with acute pancreatitis (CDHF, 2016). The peak incidence of pancreatitis for both men and women is between 40 and 70 years of age, with pancreatitis affecting men more than women in each age group (Teshima, Bridges & Fedorak, 2012, 544). In addition to age, obesity is another well known risk factor related to severe, acute pancreatitis; the "obesity epidemic" of the Western World will likely increase the incidence of pancreatitis in the future (CDHF, 2016). Using 2010 demographic data for Canada (population 34,482,779), approximately 15,100 Canadians will be newly diagnosed with acute pancreatitis every year (Teshima et al., 2012, 544).
Morbidity & Mortality
Acute pancreatitis is typically mild and resolves itself with minor complications, but it can have serious complications and a substantial mortality rate in patients with severe cases. While overall mortality from acute pancreatitis has seen steady improvements and is now at 5%, the mortality from necrotizing pancreatitis is much higher (17%), and some studies have found rates as high as 30% within the subgroup of patients with severe acute pancreatitis (Teshima et al., 2012, 545). In Canada, the average annual number of deaths due to acute pancreatitis is 300, with 10% of all acute pancreatitis deaths attributed to alcohol-induced pancreatitis (Teshima et al., 2012, 545).
Due to its location and interaction with other organs in the epigastric region of the body, many factors can contribute to and/or cause acute pancreatitis. In Canada, the most common cause of acute pancreatitis is chronic alcohol abuse, with the second most common cause being gallbladder disease (obstruction) (Lewis et al., 2014, 1191). Less common causes include trauma, post-surgical procedures, viral infections, and metabolic disorders, or pancreatitis can also be idiopathic (unknown cause) in nature.
Incidence, Prevalence, and Developmental Concerns
Pancreatitis affects 1 million Canadians, with 600,000 Canadians currently living with acute pancreatitis (CDHF, 2016). The peak incidence of pancreatitis for both men and women is between 40 and 70 years of age, with pancreatitis affecting men more than women in each age group (Teshima, Bridges & Fedorak, 2012, 544). In addition to age, obesity is another well known risk factor related to severe, acute pancreatitis; the "obesity epidemic" of the Western World will likely increase the incidence of pancreatitis in the future (CDHF, 2016). Using 2010 demographic data for Canada (population 34,482,779), approximately 15,100 Canadians will be newly diagnosed with acute pancreatitis every year (Teshima et al., 2012, 544).
Morbidity & Mortality
Acute pancreatitis is typically mild and resolves itself with minor complications, but it can have serious complications and a substantial mortality rate in patients with severe cases. While overall mortality from acute pancreatitis has seen steady improvements and is now at 5%, the mortality from necrotizing pancreatitis is much higher (17%), and some studies have found rates as high as 30% within the subgroup of patients with severe acute pancreatitis (Teshima et al., 2012, 545). In Canada, the average annual number of deaths due to acute pancreatitis is 300, with 10% of all acute pancreatitis deaths attributed to alcohol-induced pancreatitis (Teshima et al., 2012, 545).
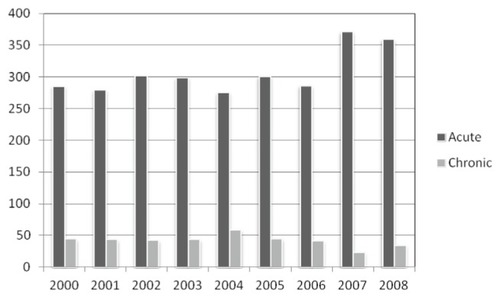
Figure 2: Average Annual Deaths from Pancreatitis in Canada
(Teshima, et. al, 2012).
Costs
Acute care inpatient costs for pancreas diseases are ranked as the 5th most expensive digestive disease in Canada costing $120 million per year, with direct health care costs related to acute pancreatitis estimated at roughly $200 million CAD per year (CDHF, 2016). The average length of hospital stay in Canada for patients with pancreatic conditions is 10 days (Teshima et al., 2012, 545). Patients with acute and chronic pancreatitis report a decreased quality of life in many areas, such as physical restrictions and often suffer from long-term mental impairments. It is difficult to assess the actual indirect costs associated with pancreatitis due to the extensive co-morbidities typical of this patient population (ie, diabetes, cardiovascular disease, smoking-related cancers, and cirrhosis) and their cumulative effect on a person’s productivity within society (Teshima et al,, 2012, 545).
Acute care inpatient costs for pancreas diseases are ranked as the 5th most expensive digestive disease in Canada costing $120 million per year, with direct health care costs related to acute pancreatitis estimated at roughly $200 million CAD per year (CDHF, 2016). The average length of hospital stay in Canada for patients with pancreatic conditions is 10 days (Teshima et al., 2012, 545). Patients with acute and chronic pancreatitis report a decreased quality of life in many areas, such as physical restrictions and often suffer from long-term mental impairments. It is difficult to assess the actual indirect costs associated with pancreatitis due to the extensive co-morbidities typical of this patient population (ie, diabetes, cardiovascular disease, smoking-related cancers, and cirrhosis) and their cumulative effect on a person’s productivity within society (Teshima et al,, 2012, 545).
